
In addition to your surgical procedure, such as a lumpectomy or mastectomy, your doctor may wish to remove and examine lymph nodes to determine whether the cancer has spread and to what extent. Your doctor will use one of two procedures for this, either a sentinel lymph node biopsy/removal or an axillary node dissection. We’ll define these terms below.
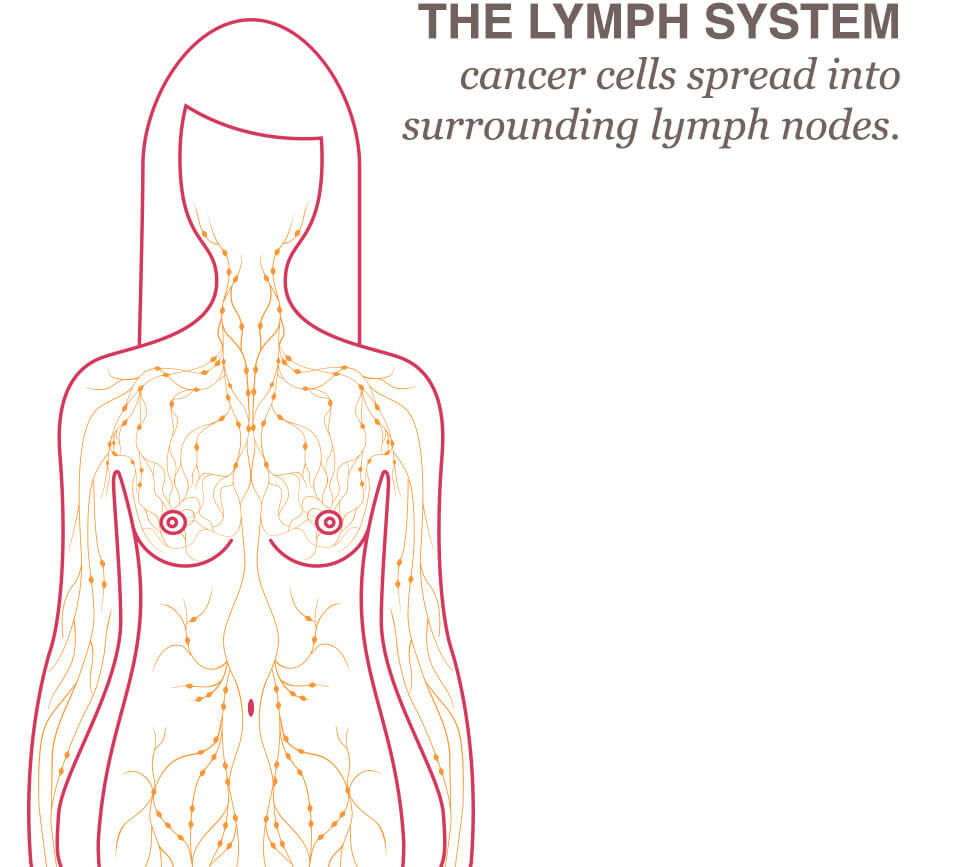
How Does The Lymph System Relate To Breast Cancer?
Although breast cancer is not easily controlled, the spread of breast cancer is sometimes predictable. The cancer cells spread through a customary path, out from the tumor and into the surrounding lymph nodes, before they progress throughout the body.
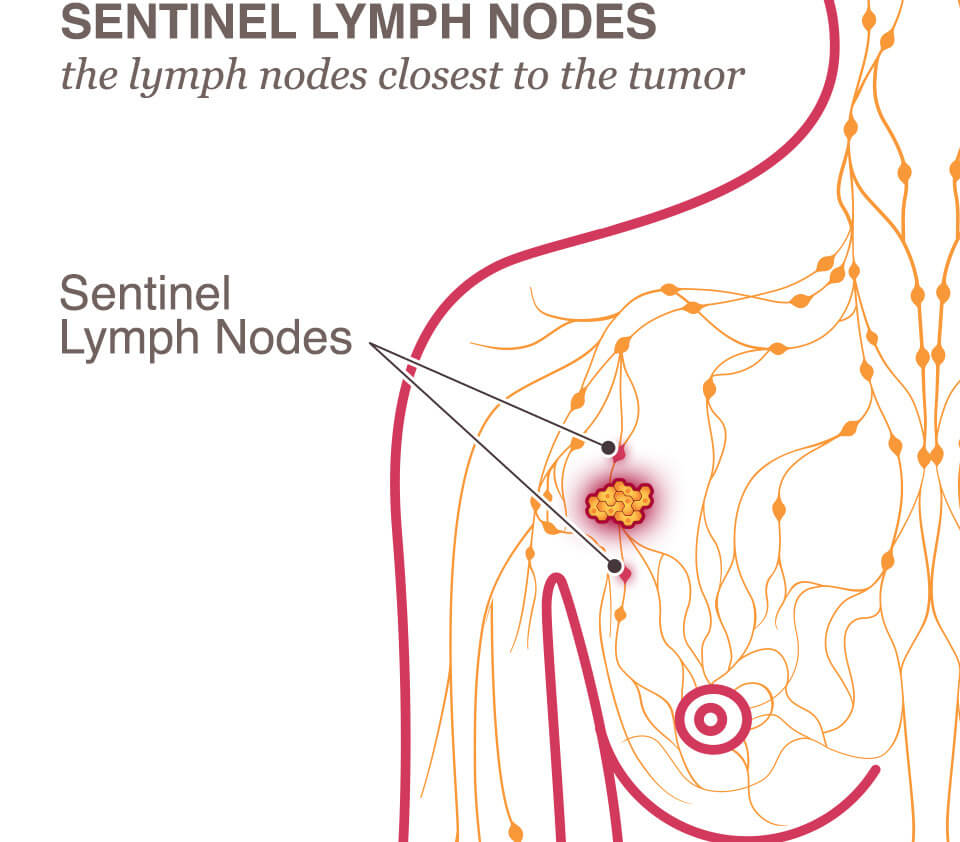
What is the sentinel node?
The sentinel lymph node (and in some cases there are several grouped together) is the first node “downstream” from the cancer in the lymph circulatory system. If the cancer were to travel away from the breast tumor and into the lymphatic system, this node would be the first one to show evidence of breast cancer.
What Is A Sentinel Node Biopsy?
A sentinel lymph node biopsy is a procedure to examine the lymph node closest to the tumor because this is where the cancer cells have most likely spread. First, the surgeon will want to identify the “sentinel lymph node,” the lymph node (or nodes) closest to the tumor. To be able to identify the sentinel lymph node, the surgeon will inject dye or radioactive substances into the tissue near the tumor. The lymph nodes that are the most susceptible to the cancer’s spread will be marked by the dye or radioactive substance. During surgery, the nearest lymph nodes will be removed and checked for the presence of cancer cells.
A biopsy is nearly always taken from the sentinel node, and the breast surgeon typically removes the sentinel node as well for dissection.
What is a Delayed Sentinel Node Biopsy?
This is a two-stage approach sometimes used in breast cancer surgery when the surgeon needs more information before removing the sentinel lymph nodes. This is particulary useful in patients undergoing breast surgery for ductal carcinoma in-situ (DCIS) or high risk lesions like LCIS, or for patients undergoing risk-reducing surgery with undetermined questionable findings on images. Here’s how it works:
1. First stage: The sentinel lymph nodes are marked during the breast surgery using a special tracer (dye) or marker, but the nodes will not be removed.
2. Second stage: After the final breast tumor pathology is received and the treatment plan clearly indicated the need to remove the sentinel nodes, the surgeon performs the delayed sentinel lymph node removal as a second procedure. They locate the previously marked nodes and remove them to check for the presence of cancer cells.
Advantages of delayed sentinel node biopsy
- To avoid removing nodes unnecessarily before knowing if this procedure is required.
- To lower the risk of complications like arm swelling (lymphedema) by limiting the unnecessary removal of nodes.
Dr Alazhri has a special interest in this procedure. She has developed several innovative techniques that were published and presented at international conferences.
What Is An Axillary Node Dissection?
This is a procedure by which the breast surgeon removes some of the axillary lymph nodes, which are the lymph nodes located in the underarm. Once removed, they are dissected and examined.
Do The Lymph Nodes Always Need to Be Removed?
Not always, especially when there is no evidence of any cancer in the lymph system. The decision whether or not to remove any lymph node is tailored to each patient and thoroughly discussed at a multi-disciplinary tumor board (MDT) meeting.
In patients over the age of 50, with small, low risk tumors, axillary surgery may be omitted, while sentinel node biopsy is recommended for the remaining group of patients with invasive breast cancer.
Following sentinel node biopsy, the pathologist will test the lymph nodes to determine whether the cancer has spread past the breast. When some evidence of cancer is found in the lymph system, recent standards are as follows:
- Effective in mid-2012, the standard of care was changed to no longer require women with early stage breast cancers and metastasis to one or two axillary lymph nodes to have a full dissection and removal of the lymph nodes under the arm. Instead radiation to the underarm can be planned.
- For patients with more than 2 diseased sentinel lymph nodes, or locally advanced breast cancer (not early), axillary nodal dissection is the standard of care.
- For patients who received chemotherapy before surgery (neoadjuvant chemotherapy):
- If they had no clinical evidence of nodal disease, sentinel node biopsy can be performed.
- If they had an evidence of nodal disease at the time of surgery, the decision of axillary node dissection depends on the size of metastasis in the node, and is usually discussed at the MDT meeting.
- If they had an evidence of nodal disease before chemotherapy and it improved after chemotherapy, sentinel node biopsy may be performed using special modified techniques, to improve accuracy and detection.
